
6 results
Changing trends of suicide mortality from 2011 to 2019: an analysis of 38 European Countries
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S85-S86
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Suicide is a serious public health problem since it accounts for nearly 900,000 deaths each year worldwide. Globally in 2019, 10.7 persons out of 100,000 died by suicide. Psychiatric disorders are related to an overwhelming proportion of these cases. In the last years, several specific interventions and action plans for suicide prevention have been implemented in a number of European countries.
ObjectivesOur aim was to analyze recent epidemiologic trends of suicide mortality rates in Europe.
MethodsAnnual national statistics of suicide mortality rates derived from Eurostat public databases from 2011 to 2019 were analyzed for 38 European countries. The suicide mortality rate was estimated per year/100,000 population. Linear regression models were used to study temporal trends of suicidal mortality. Analyses were performed using RStudio.
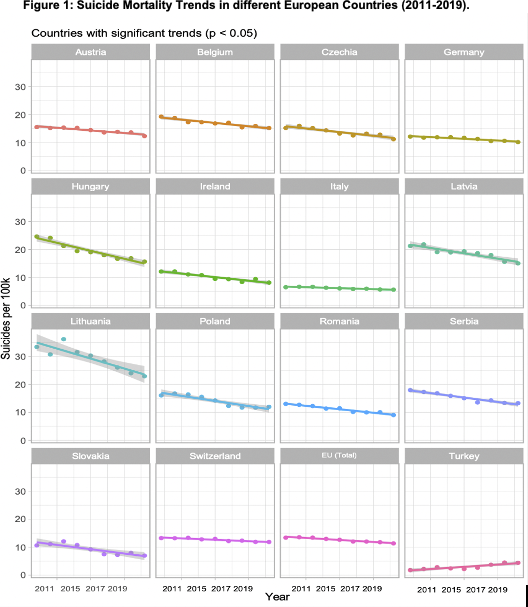
ResultsAvailable data show a statistically significant reduction in suicide mortality rates from 2011 to 2019 in 15 European countries, and a significant increase for Turkey (ES=0.32, SD=0.06, p=0.037) (Fig 1). The greatest significant decrease was reported in Lithuania (ES=-1.42, SD=0.02, p=0.02), followed by Hungary (ES=-1.13, SD=0.11, p=0.0007), Latvia (ES=-0.76, SD=0.11, p=0.007), and Poland (ES=-0.73, SD=0.10, p=0.001). Italy reported the lowest significant reduction in suicide mortality rates (ES=-0.13, SD=0.018, p=0.003). The remaining 16 countries showed no significant changes in suicide mortality trends.
Image:
 Conclusions
ConclusionsIn the last years, Europe registered an overall reduction in reported suicide rates. However, more recent data (i.e., suicide rates after COVID-19 pandemic, age and sex-related effect on suicide rates) should be analyzed and used to implement future recommendations. Current and future suicide prevention strategies aim to contribute to a greater reduction of suicide rates in the different European countries.
Disclosure of InterestNone Declared

Recovery from DSM-IV post-traumatic stress disorder in the WHO World Mental Health surveys
-
- Journal:
- Psychological Medicine / Volume 48 / Issue 3 / February 2018
- Published online by Cambridge University Press:
- 19 July 2017, pp. 437-450
-
- Article
- Export citation
The cross-national epidemiology of DSM-IV intermittent explosive disorder
-
- Journal:
- Psychological Medicine / Volume 46 / Issue 15 / November 2016
- Published online by Cambridge University Press:
- 30 August 2016, pp. 3161-3172
-
- Article
- Export citation
Barriers to mental health treatment: results from the WHO World Mental Health surveys
-
- Journal:
- Psychological Medicine / Volume 44 / Issue 6 / April 2014
- Published online by Cambridge University Press:
- 09 August 2013, pp. 1303-1317
-
- Article
- Export citation
Mood and anxiety disorders across the adult lifespan: a European perspective
-
- Journal:
- Psychological Medicine / Volume 44 / Issue 4 / March 2014
- Published online by Cambridge University Press:
- 31 May 2013, pp. 707-722
-
- Article
- Export citation
Cross-national differences in the prevalence and correlates of burden among older family caregivers in the World Health Organization World Mental Health (WMH) Surveys
-
- Journal:
- Psychological Medicine / Volume 43 / Issue 4 / April 2013
- Published online by Cambridge University Press:
- 09 August 2012, pp. 865-879
-
- Article
- Export citation
